Dr Ross Kerridge is the Senior Staff Specialist in Anaesthesia & Perioperative Service, John Hunter Hospital, and Conjoint Associate Professor, Anaesthesia & Perioperative Medicine at the School of Medicine & Public Health, University of Newcastle. This is an abridged version of a presentation given at the International Symposium on the History of Anesthesia in Sydney in 2013. For the full version, please see Proceedings of the 8th International Symposium on the History of Anesthesia.
The community and its hospital
Newcastle in the 1950s was an industrial city. The steelworks, ship building and associated industries centred on the port and set the character of the city. There was no national health insurance system at the time, and the highly unionised workforce, working in large groups, fostered the development of community-wide approaches to the organisation of health insurance. An innovative hospital-based health insurance system was established at the Royal Newcastle Hospital. The public could make regular contributions to a fund held by the hospital, for which they were able to receive their comprehensive medical care through the institution and its various branches. This innovative model set the pattern for later development around the world of what are commonly referred to now as health maintenance organisations. The funds acquired by the hospital through the patient contribution scheme facilitated the development of new systems of hospital organisation, both clinical and non-clinical. Among these changes was the development of a new system of medical staffing for the hospital. The unusual developments were led by the inspiring but controversial Dr Chris McCaffery, the general superintendent of the hospital from 1940-1955. Many of McCaffery’s ideas, pioneered during the 1940s and 1950s, later became generally accepted around the world, but others remain controversial.
The Medical and Nursing Staff
At the end of World War II (WWII), McCaffery recruited promising and innovative doctors leaving military service to join the hospital in developing a new approach to medical care. The doctors were employed full-time as salaried hospital staff. The hospital also established a three year medical residency program for new graduates modelled on the major American institutions – a complete innovation within Australia. This training program proved to be very attractive, and enabled the Newcastle hospital to attract some of the academically superior graduates away from the prestigious established Sydney hospitals.
There was positive encouragement of innovation, iconoclasm, and an accepted ethos of challenging established ideas. In parallel with these medical staff changes, the nursing leadership developed professionalisation and increased education for the nursing staff. These factors worked together to foster an attitude of willingness to try new approaches to the treatment of patient illness.
The Medical Individuals
The leading clinician involved in this case was Ivan Schalit. Schalit was the first full-time director of anaesthesia in Australia. He was recruited to the hospital at the end of the war, attracted by the clinical and intellectual freedom offered by a full-time salaried position. He was also an idealistic socialist, although in later life felt socialism was impossible because of human greed. Warren Gunner was the hospital’s first anaesthetics registrar, and thus worked closely with Schalit. Bill Cumming was the youngest doctor (what would now be called the intern), and became most closely involved with the continuous care of the patient.
The Clinical Problem
During the 1950s, the lack of effective contraception meant unwanted pregnancies were frequent. In Australia, as in most countries throughout the world, abortion was a criminal act. Nevertheless, abortions were common. Available data suggests that more abortions were performed per woman than is currently the case in Australia today. Procuring an abortion was a criminal act by both the proceduralist and the woman. Inevitably, this led to delayed presentation if there were complications, difficulties in gaining an accurate history from the patient, and challenges in medical management.
It is still difficult to obtain a clear picture of exactly what happened, even by speaking to those who were working as doctors and nurses at the time. ‘Women of means’ were able to obtain abortions performed discreetly by some cooperative doctors. Those with less means would go to ‘clinics’ run by nurses or others with some training, and gain abortion with varying degrees of skill and safety. An abortion clinic ran for some years immediately across the road from the Royal Newcastle Hospital’s emergency department, using sterile theatre instruments borrowed, illegally and for a payment, by unidentified hospital staff. Local legend also reports a butcher in the working class suburb of Tighes Hill provided abortions for some time during the 1950s. Other women used other means including a variety of ‘home remedies’.
Abortions in Newcastle were commonly performed on Fridays. As the story goes, the large industries paid their workers on Thursday, and that night or the following morning, women in need would go to the abortion clinic and then report to the emergency department with ‘unexplained’ vaginal bleeding, stating they may be pregnant. They would not admit to having done anything to cause it, and would not reveal where it had been done. Attempting to procure an abortion was a criminal offence. A retired nurse recalls she “…used to hate working in casualty on Friday evenings, because that’s when they would come in”.
The Case
On 21 April 1955, a 22 year old married women was admitted to Royal Newcastle Hospital with a history that she had made two attempts, on the 18 & 20 April, to terminate a pregnancy presumably by using a syringe, which caused physical trauma through the cervix, and inserting soapy fluid. Her last menstrual period was mid-January. The patient was now febrile with a foul discharge from the cervix. As was standard procedure at the time, the case was treated as an infected miscarriage and curettage was not performed.
The next day she had lower abdominal tenderness but no rigidity. At 4am on 23 April, the first symptoms of tetanus became evident with stiffness of her jaw and soreness of her neck. This rapidly progressed so that by 7am she had marked neck stiffness, abdominal rigidity and risus sardonicus, (a fixed tense grin, typical of tetanus). At this time sedation was given initially with intramuscular phenobarbitone plus intravenous thiopentone. Simultaneoulsy anti-tetanus serum was administered both intravenously, and intramuscularly. After examination under general anaesthesia and dilation of the cervix (but not curettage) to allow drainage of the uterus, anti-tetanus serum was injected into each parametrium. At 4pm, twelve hours after the onset of trismus, the patient began having convulsions. Sedation was increased until there was respiratory depression between convulsions accompanied by cyanosis.
In this setting of the patient in extremis, the decision was then made to curarise, intubate and ventilate the patient. The patient was initially ventilated using manual intermittent positive pressure ventilation on the bellows of an Oxford vaporiser.
When interviewed many years later, Gunner described these events as a rapidly progressive stream of increasingly dramatic medical interventions. He recalled that ‘suddenly’ he and Schalit found themselves with a patient curarised and being mechanically ventilated, and then had to think “what do we do now?”. They were not sure at that point how long the patient would survive, whether she would survive, and how they were going to manage the situation.
Faced with this situation, Schalit then assembled the necessary items to produce a mechanical ventilator using anaesthetic apparatus, personal household kitchen and laundry appliances, and his young son’s meccano set. This was an ongoing work involving trial and error for at least the first few days. He was assisted by Rod Earp Snr, a non-medical friend who was “handy” with mechanical things. The electric motor was obtained by adapting a small household ‘clothes press’ used for squeeze-drying small towels etc. Years later, Schalit’s wife Nina commented “Fortunately, the patient survived….Unfortunately my clothes press did not.”
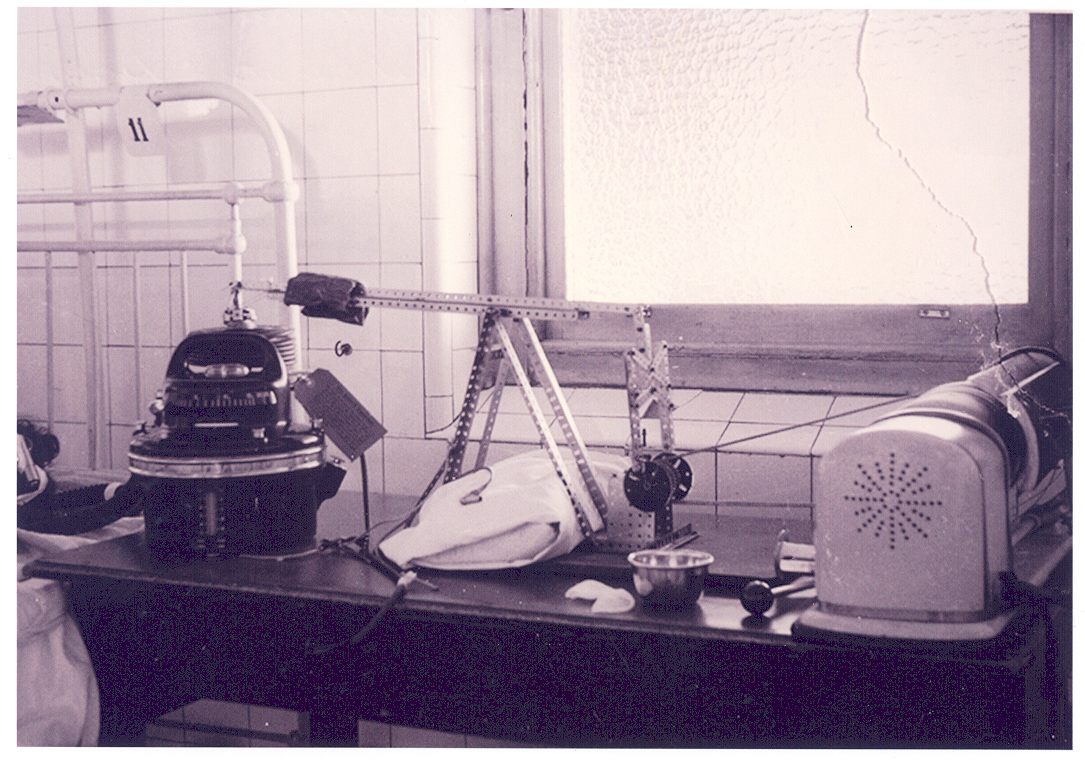
Image caption: The “Meccano Ventilator”. The apparatus was constructed from a household device for squeeze-drying/ironing items such as small towels etc. It was used to provide the drive-power that was modified through the levers and gears to drive the concertina bellows.
Sedation and curarisation were maintained to control convulsions, ensure muscular flaccidity and enable adequate ventilation. Tracheostomy was performed on the second day to facilitate suction and a stable airway without laryngeal irritation. When the patient had been fully curarised sedation was not given for two days. It was then noted that the patient was conscious and could move a finger or toe upon demand, and sedation was recommenced.
The detailed description in the Medical Journal of Australia (MJA) includes description of many very basic aspects of clinical care that would now be considered routine, but were lessons learnt de novo while treating this patient.
A Ryles tube was passed, although not specified whether it was oral or nasal, to enable sedation with enteral phenobarbitone rather than intramuscularly. Nutrition was not given by the tube because of concern about regurgitation. Intravenous nutrition was supplied using ethanol and glucose.
In contrast to the report by Lassen et al, the group in Newcastle chose not to use a Boyle’s anaesthetic machine. Rather, the patient was ventilated using an Oxford bellows drawing air from the atmosphere. It is not clear from the report why this decision was made, but seems to represent a shift away from ‘anaesthetising’ the patient to treating the patient using ‘anaesthetic principles’ – as reflected in the title of the report.
A deliberate decision was made to ventilate using air rather than oxygen. This was to avoid the use of high concentrations of oxygen because it would mask any obstruction of the airway. There was also consideration of the “possible danger of oxygen poisoning”. Reading the text, it appears that the authors are referring to atelectasis.
The decision to use air may have had other benefits. In other centres, where long-term ventilation was provided using an anaesthetic machine, the gas mixture was oxygen and nitrous oxide. The toxicity of nitrous oxide was not known at the time, although was reported shortly afterwards. In Lassen’s paper in late 1954, he notes the development of haematological effects including granulocytopaenia, but does not attribute this to nitrous oxide. Lassen had earlier suspected curare as the cause, but in 1956 nitrous oxide was implicated as the cause of fatal bone-marrow depression; something worked out by Dr Pat Mackay while working at the Royal Melbourne Hospital. While fortunate for the patient, it is unclear if Schalit had anticipated this concern in 1955.
Humidification was recognised to be a problem and in the MJA report, the authors note that “despite many experiments, no method appeared to be wholly satisfactory”. An interview with Cumming in 2011 suggests this understates the problems. At one point the patient developed acute respiratory obstruction and became deeply cyanosed while this was being dealt with. Eventually, when the patient was in extremis, a hardened mucous plug with a clear ‘structure’ reflecting the bronchial anatomy was removed from the patient’s airway, and ventilation was re-established. Even 60 years later, he recalled it as one of the most dramatic events of his long career, and one moment when the patient’s outcome was particularly at risk.
Cumming recalls another major drama in terms of ventilatory control which occurred when there was a total electrical failure in the hospital. Although there were manual means to ventilate the patient, the total blackout made things difficult, and when the power was eventually re-established the woman was deeply hypoxic.
Curarisation was able to be ceased after twelve days, and sedation with barbiturates was then given to control convulsions from that time. Active mechanical ventilation was continued until twenty six days. At that time it was weaned and in the MJA paper this time was described as providing the most anxious moments of the illness. Curiously, Cumming did not describe it this way when interviewed 60 years later. He remembered it was a time of gradually getting the patient to breathe without the assistance of the machine and gradually increasing the time the patient was breathing for herself.
This process took about three days, and the patient was then able to breathe spontaneously via the tracheostomy. From the thirty-eighth day, the tracheostomy tube was progressively blocked until it became clear it was no longer needed. Sedation was gradually reduced and then the tracheostomy tube was removed.
After the patient recovered, the regular clinical quality meeting at the hospital was used to present the case to the medical staff. Unusually for the time, the patient was invited to come along and discuss her recall of the case. She reported she was aware but confused during most of the period of ventilation. Although the patient later complained to the hospital about her tracheostomy scar.
Initially, many of the hospital’s doctors felt the treatment was an inappropriate intervention in a hopeless case. The case was not the first time a tetanus patient had been treated in this way internationally, and when interviewed by the author Gunner recalled that some cases had been similarly treated in Melbourne (though not in Sydney). The Newcastle case was, however, more severe and prolonged than previously reported cases. As the case progressed, most of the hospital became interested in the work that was being done. The ultimately successful outcome attracted wide attention nationally and became one of the legends of the hospital. The legend included humorous recall of the “Meccano Set Ventilator”, as well as the attendance by the patient (and her appearance) at the clinical meeting.
Outcome
The experience gained in this case provided the basis for the later development of an intensive care unit in Newcastle. In particular, a cohort of senior nurses who had experience and familiarity with the challenges of ventilation, prolonged curarisation, and the principles of mechanical ventilation were produced. This group later became senior nurses in the hospital, and helped establish the intensive care unit in the hospital.
The subsequent life of the patient is not known. A nurse recognised her in public some time later, but the patient avoided contact. A woman of the same age and with a very similar name was treated at the hospital after a spontaneous miscarriage in 1962, but no detailed health records have been found from this admission.
The Royal Newcastle Hospital continued to be a centre of innovation, both in clinical care and in organisational aspects of health care. At times this was intensely political and controversial, leading to the board of the hospital being dismissed twice, once in 1965 and again in 1991. In 1990 the bulk of the hospital was moved to a new campus as the John Hunter Hospital. The move was completed in 2006, accompanied by celebrations of the hospital’s history.
Warren Gunner went on to have a notable career at St Vincent’s Hospital in Sydney, establishing the intensive care unit there, and worked closely with Sir Harry Windsor in cardiac surgery. He was a keen photographer as a young doctor and rediscovered the photos of the patient and ventilator amongst his collection in 2005. The discovery of these photos stimulated my interest in the case and I was privileged to be able to interview him shortly before his death.
Bill Cumming, the junior doctor of the team, later became professor of orthopaedic surgery at St George Hospital in Sydney.
Ivan Schalit remained as the director of anaesthesia in Newcastle until 1968. He then stepped back from this role but continued working in the hospital for some years. He is remembered as a “gentleman of the old school” personally, and as a skilled but humble anaesthetist who delighted in his work and teaching.
Today, we understand more, have better drugs and equipment, and routinely manage cases much more physiologically complex than this one. But while we see more, it is by standing on the shoulders of giants.
List of References
Duggan JM, Hendry PIA, ‘Royal Newcastle Hospital: the passing of an icon’, Medical Journal of Australia, 2005, 183, pp642-645
Gunner BW, Cumming WJ, Schalit I, ‘The Employment of Anaesthetic Principles in the Management of a Severe Case of Tetanus’, Medical Journal of Australia, 1956, pp402-404
Honey GE, Dwyer BE, Smith AC, Spalding JM, ‘Tetanus treated with tubocurarine and intermittent positive-pressure respiration’, British Medical Journal, 1954, Vol 2, Issue 4885, pp442-3.
Lassen HCA, ‘A preliminary report on the 1952 epidemic of poliomyelitis in Copenhagen with special reference to the treatment of Acute Respiratory Insufficiency’, Lancet, 1953, Vol 1, pg37
Lassen HCA, Bjorneboe M, Ibsen B, Neukirch F, ‘Treatment of Tetanus with curarisation, general anaesthesia, and intratracheal positive-pressure ventilation’, Lancet, 1954; Vol 2, pg1040
Macourt D. ‘Incomplete Abortion: an analysis of one method of management’, Medical Journal of Australia, 1966, Vol 2, pp640-2.
Saint EG, Joske RA, Stubbe JL, ‘The Treatment of Tetanus’, Medical Journal of Australia, 1953 Vol. 1, Issue 11, pp361-4
Wilson P, Martin FIR, Last PM, ‘Bone-Marrow depression in tetanus. Report of a fatal case’, Lancet, 1956 Vol 271, pp442-443
Personal communication with Billy Cummings
Personal communication with Nina Schalit, 2013.
Personal communication with Allan Hewson
Personal communication with nurse Dr Betty Capper
Personal communication Hughes 2013
Personal communication with Bill Gunner 2008