THE SCIENCE OF MEDICINE
Plant-based medicine was unpredictable. Plant potency was related to geographical location. Variations in preparation also produced inconsistent strength and reliability in medicines.
Doctors of the Hippocratic or Galenic traditions considered themselves scientific. The diagnoses and therapies they offered sat comfortably within their rational understandings of the world.
These were justified through experience.
Experience suggested bloodletting helped, “wandering womb” was an illness, and tooth decay was caused by worms burrowing into teeth.
Throughout the 19th Century, medicine matured, looking to science to achieve reproducible results in a laboratory setting. Alkaloids were isolated from traditional medicinal plants, synthetic drugs were produced, germ theory was established and understandings of human anatomy were gained from the human body. Folkloric medicine was displaced by scientific medicine.
COLLEGE COAT OF ARMS
The shield on the College coat of arms is filled with plants of importance to the development of anaesthesia and pain medicine.
The upper half of the shield holds plants representing the “old world”.
Opium and mandrake are used to signify analgesia, sedation and anaesthesia. Medicinal use of these plants is recorded in antiquity and was widespread. Archaeologists have discovered poppy seeds at Neolithic sites, circa 30,000 BCE.
The lower half of the shield represents the “new world”, with curare, and coca leaf and fruit.
Curare and coca have been used in South America for millennia. Curare was used to immobilise and kill prey, and became the foundation for developing muscle relaxants.
More information about the coat of arms can be found on the ANZCA website.
CURARE
Chondrodendron tomentosum
Deep in the Amazon jungle, indigenous people once hunted using blow guns with poison darts dipped in resin from Chondrodendron tomentosum roots. The roots were ground to paste with other herbs and poisons. Curare paralyses muscles, shutting down the respiratory system.
In the 19th Century artificial ventilation was used to keep curarized animals alive. Later experiments showed curare acted at the nerve-muscle junction.
Seeking to cure his multiple sclerosis, Richard Gill (1901 – 1958) gave 25 pounds of crude curare to the pharmaceutical company E. R. Squibb & Sons. They didn’t develop the hoped for cure but did standardise curare, creating a neuromuscular blocking agent, dramatically changing anaesthesia practice.

INTOCOSTRIN
During the 19th Century curare was unsuccessfully used to treat rabies, tetanus and epilepsy. By 1935, Harold King had isolated tubocurarine, curare’s active ingredient. In 1942, Harold Griffith successfully used standardised curare (Intocostrin) with cyclopropane. Within five years synthesised muscle relaxants were available.

ELECTRO SHOCK THERAPY
In 1940 doctors started experimenting with curare for use with electric shock therapy. Electric shock therapy regularly caused broken bones, including vertebrae, and all sorts of dislocations. The intensity of convulsions was high and couldn’t be controlled. Intocostrin, combined with an anaesthetic agent, was a break-through for this treatment.
MANDRAKE
Mandragora officinarum
Mandragora is native to southern Europe. Pedanius Dioscorides, a Greek physician and surgeon in Nero’s army, used the word anaesthesia to describe the absence of sensation mandrake produced.
Mandrake is from the nightshade family, related to potatoes and parsnip. It has been associated with the mystical, magical and medicinal since ancient times.
Strange beliefs surrounded mandrake. It has been used as an aphrodisiac, to exorcise demons and, in 1630, as proof three women from Hamburg were witches. Mandrake was also said to shriek in a way that could kill anyone trying to uproot it (see Harry Potter for handling shrieking mandrake).

XYLOCAINE
Xylocaine is an anaesthetic released onto the market in 1948. It was developed following a twist in research into certain mutations of barley during a search for an industrial pesticide. It works by preventing nerves from transmitting painful impulses to the brain, causing loss of feeling during dental or surgical procedures.

EVIPAN
Evipan is a barbiturate derivative having hypnotic and sedative effects. It was introduced as an agent for inducing anaesthesia is 1932, and continued to be used until the 1950s. It could be difficult to control the depth of anaesthesia, which made it quite dangerous.
PITURI
Duboisia Hopwoodii
Duboisia hopwoodii grows throughout the Australian interior and was collected and traded by Aboriginal Australians. Its effects varied, with some colonial reports saying it was a stimulant, while others claimed a narcotic effect. 20th Century analysis has revealed both nicotine and nornicotine, depending on the region of origin.
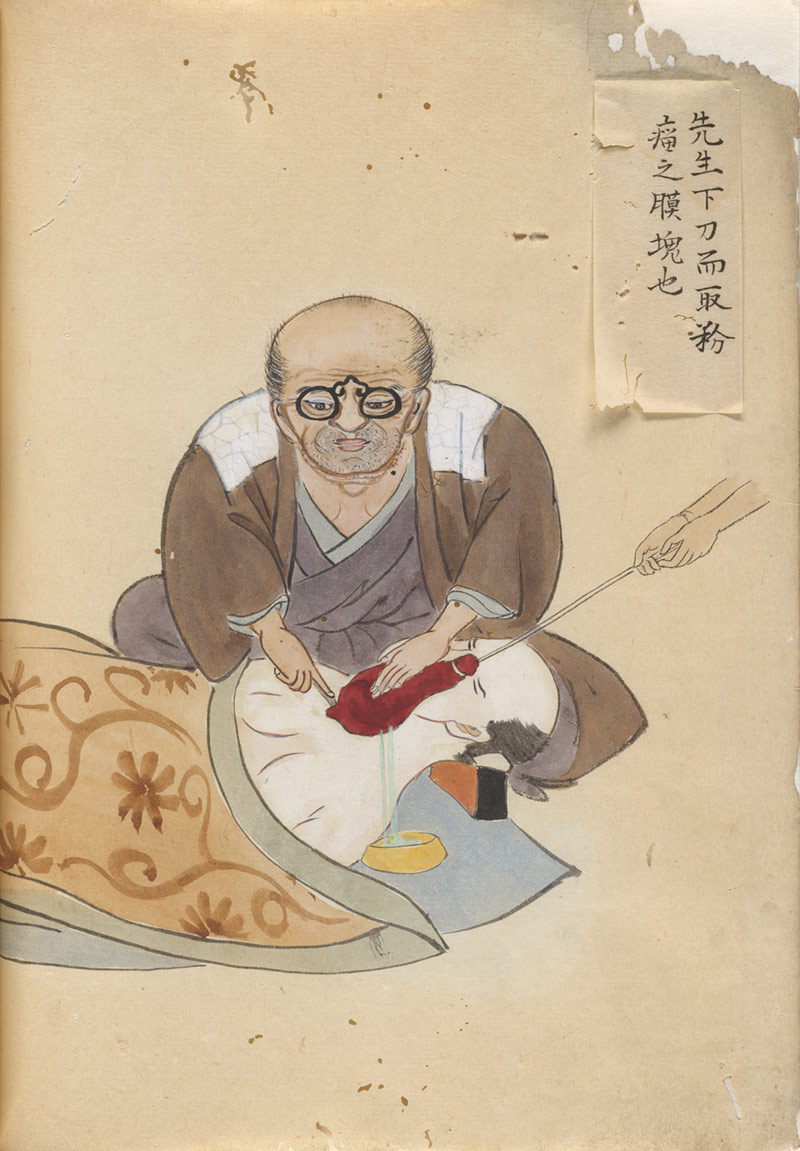
SEISHA HANAOKA
Datura stramonium
In 1804, Seisha Hanaoka, a Japanese surgeon, administered a potent mixture of alkaloids to a woman prior to an operation. Datura stramonium, or Devil’s Trumpet, produced hours of complete unconsciousness. He called this mixture Tsusensan and successfully used it on many patients.

COCA LEAF
Erythroxylum novogranatense var. novogranatense
Amara Indians in Peru have used coca leaf for thousands of years. The leaves are primed with ash, formed into a wad and dried, then chewed or sucked. The process can be repeated several times a day.
Few Europeans knew cocaine existed until Sigmund Freud published Über Coca in 1884. Freud’s paper praised cocaine as a miracle drug and also noted it ‘had a marked anesthetizing effect’. Freud’s contemporary, Carl Koller, an ophthalmologist from Vienna, recognised the value of this effect and realised its potential as a local anaesthetic.
In Peru, coca was used to energise, stave off hunger and keep people warm. In 19th Century Austria it was also found to have an anaesthetising effect.

SPINAL ANAESTHESIA
1884
Following Koller’s discovery of local anaesthesia, American surgeon William Halsted experimented with cocaine for spinal anaesthesia. While his experiments were successful, in the process he developed cocaine addiction. In an attempt to rid himself of this addiction, Halsted was subjected to substitution therapy, leading to morphine addiction.

STOVAINE
1904
Ernest Fourneau manufactured the local anaesthetic Stovaine in Paris. It was non-addictive, could be applied topically or injected and used for spinal anaesthesia. However, there were limitations. Stovaine produced pain on injection, tissue oedema, irritation, necrosis and “after-pain”.
SYNTHETIC DERIVATIVES OF COCAINE
Novocain (Procaine) was used by dentists as a less addictive alternative to cocaine. It had a longer duration of action but carried a higher risk of allergic reaction. The use of Novocain declined with the introduction of lidocaine in the late 1940s. By the 1980s Novocain was almost phased out completely.
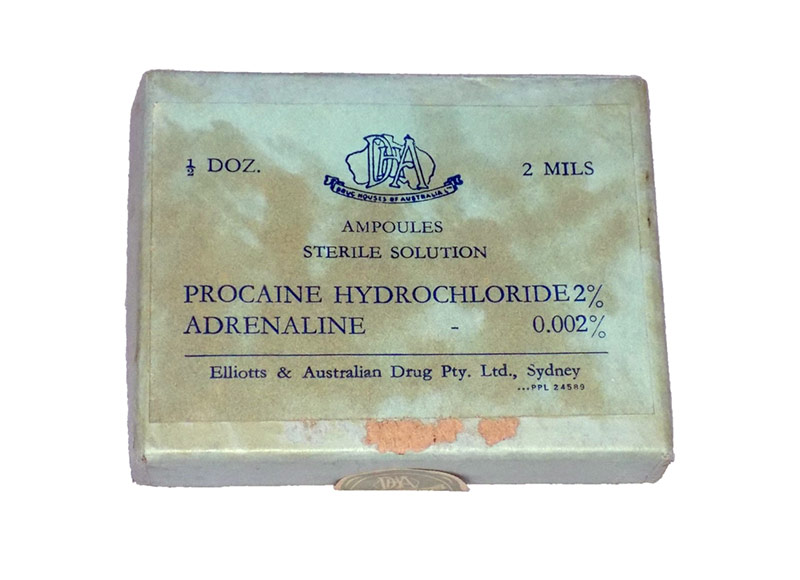
PROCAINE
1904
Procaine was developed in 1904. It was the first synthetic derivative of cocaine for use as a local anaesthetic. It was introduced to the market under the trade name Novocain. Procaine had low toxicity, was less irritating than cocaine and non-addictive.

NOVOCAIN
1905
The safety of Novocain increased the scope of local anaesthesia. It was soluble in water, stable enough to boil and could be combined with adrenaline. In 1908, August Bier described an arm block using intravenous procaine and a tourniquet.
OPIUM
Searching for ultimate pain relief
The Sumerians referred to opium as Hul Gil, the “joy plant”. During the Inquisition, opium disappeared from Europe. Anything associated with the East was linked to the devil. In 1527 it was reintroduced by Paracelsus as laudanum. Mixed with citrus juice and gold, it was produced as “stones of immortality”; black pills that were powerful painkillers.
When morphine was isolated, it was called “God’s own medicine” for its reliability, long-lasting effects and perceived safety.
In 1874, English researcher C.R. Wright boiled morphine and created diacetylmorphine. 21 years later The Bayer Company of Germany diluted morphine with acetyls, also producing diacetylmorphine. They called it “heroin”, but didn’t introduce it commercially for another three years.

OMNOPON
c.1930
Omnopon is a mixture of hydrochloride salts of opium alkaloids. It was used to relieve moderate to severe pain and for pre-operative sedation.
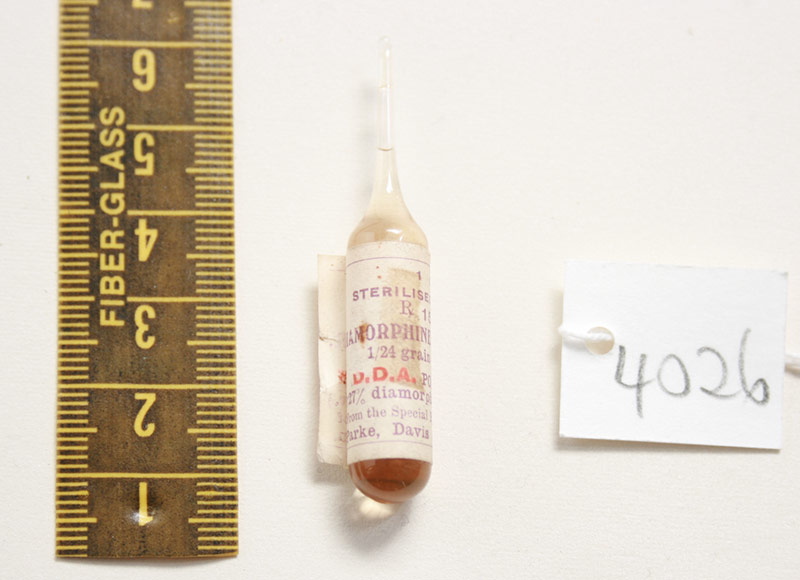
DIAMORPHINE HYDROCHLORIDE
First discovered in 1874, heroin was used as a pain reliever and in substitution therapy for cocaine and morphine addiction. Its highly addictive qualities were not revealed until much later and it was widely available. Heroin is still used in some countries for pain relief in terminal illnesses.
MORPHINE
Morphine was isolated in 1817. In 1843, Dr Alexander Wood of Edinburgh discovered a new technique of administering morphine, injection with a syringe. Injecting his patients directly in painful areas, he found morphine provided instantaneous relief, and was three times more potent than when administered orally.
The concept of the syringe wasn’t new, Galen had used one to inject blood vessels of the brain. With the invention of the hollow needle, by Irishman Francis Rynd in 1844, and the design of a practical metal syringe by Charles Pravaz in 1853, the skin no longer needed to be cut prior to being injected.

PRAVAZ SYRINGE
1853
This small, ornate syringe is made of silver and could be used with a hollow needle to inject medicines directly under the skin.

MORPHINE SYRINGE KIT
1930
The development of the syringe provided the perfect method for administration of morphine. Doctors regularly carried their own syringe kits. Needles and syringes were sterilised and reused.